
Translate this page into:
Advancements in Extracorporeal Therapies for Managing Sepsis: A Comprehensive Review

*Corresponding author: Prafulla Karbhari Doifode, Department of Internal Medicine, Max (Alexis) Superspeciality Hospital, Nagpur, Maharashtra, India. prafulladoifode7210@gmail.com
-
Received: ,
Accepted: ,
How to cite this article: Doifode PK, Ramteke V, Dambhare N. Advancements in Extracorporeal Therapies for Managing Sepsis: A Comprehensive Review. Vidarbha J Intern Med. doi: 10.25259/VJIM_16_2024
Abstract
Sepsis remains a critical condition associated with high morbidity and mortality rates despite advances in medical care. The dysregulated host response to infection leads to systemic inflammation and multi-organ dysfunction, often exacerbated by a cytokine storm involving both proinflammatory and anti-inflammatory mediators. Extracorporeal therapies have emerged as potential adjuncts in sepsis management, aiming to mitigate the inflammatory response and support vital organ function. These therapies include various modalities such as adsorption of inflammatory mediators, removal of endotoxins and cytokine clearance using specialised filters and devices. This review explores the principles, mechanisms and clinical evidence surrounding extracorporeal therapies in sepsis, highlighting their potential benefits and current limitations. Key devices discussed include polymyxin B haemoperfusion, CytoSorb haemoadsorption, high-volume hemofiltration and novel technologies such as the oXiris membrane and Seraph-100 Microbind Affinity Blood Filter. Clinical trials and studies assessing these therapies provide insights into their efficacy in improving haemodynamics, organ function and mortality outcomes in septic patients. Despite promising results in certain trials, variability in patient responses and conflicting evidence necessitate further research to refine treatment protocols and optimise patient selection criteria for extracorporeal therapies in sepsis.
Keywords
Sepsis
Extracorporeal therapy
Cytokine storm
Haemoadsorption
Hemofiltration

SEPSIS
Sepsis is defined as a life-threatening organ dysfunction associated with a dysregulated host response to an infection. It is a severe multi-organ syndrome caused by an infection and is associated with increased morbidity and mortality.[1] Septic shock is a subtype of sepsis where there is vasopressor requirement to maintain a mean arterial pressure of 65 mmHg or more and serum lactate level >2 mmol/L (>18 mg/dL) in the absence of hypovolemia. Septic shock carries a higher mortality risk compared to sepsis.[2] A cytokine storm is a harmful immune system response involving an imbalance of proinflammatory cytokines (Interleukin [IL]-1, IL-6, IL-17 and tumour necrosis factor-alpha [TNF-α]) and anti-inflammatory cytokines (IL-4, IL-10 and transforming growth factor beta) leading to excessive cell stimulation, inflammation and consequent organ dysfunction.[3]
Pathogens after invasion in body, expresses certain molecular patterns or endotoxins called pathogen-associated molecular patterns (PAMPs) and damage-associated molecular patterns (DAMPs) lead to the dysregulated activation of macrophages, T-cells, neutrophils and variety of cells. It, in turn, leads to activation of inflammatory cytokines leading to tissue and organ damage [Figure 1].[4] Its symptoms vary from fever, fatigue, myalgia, arthralgia, headache, rash, diarrhoea, anorexia to renal failure, acute liver injury, stress-related takotsubo-like cardiomyopathy and/or death depending on the severity of infection.[5]
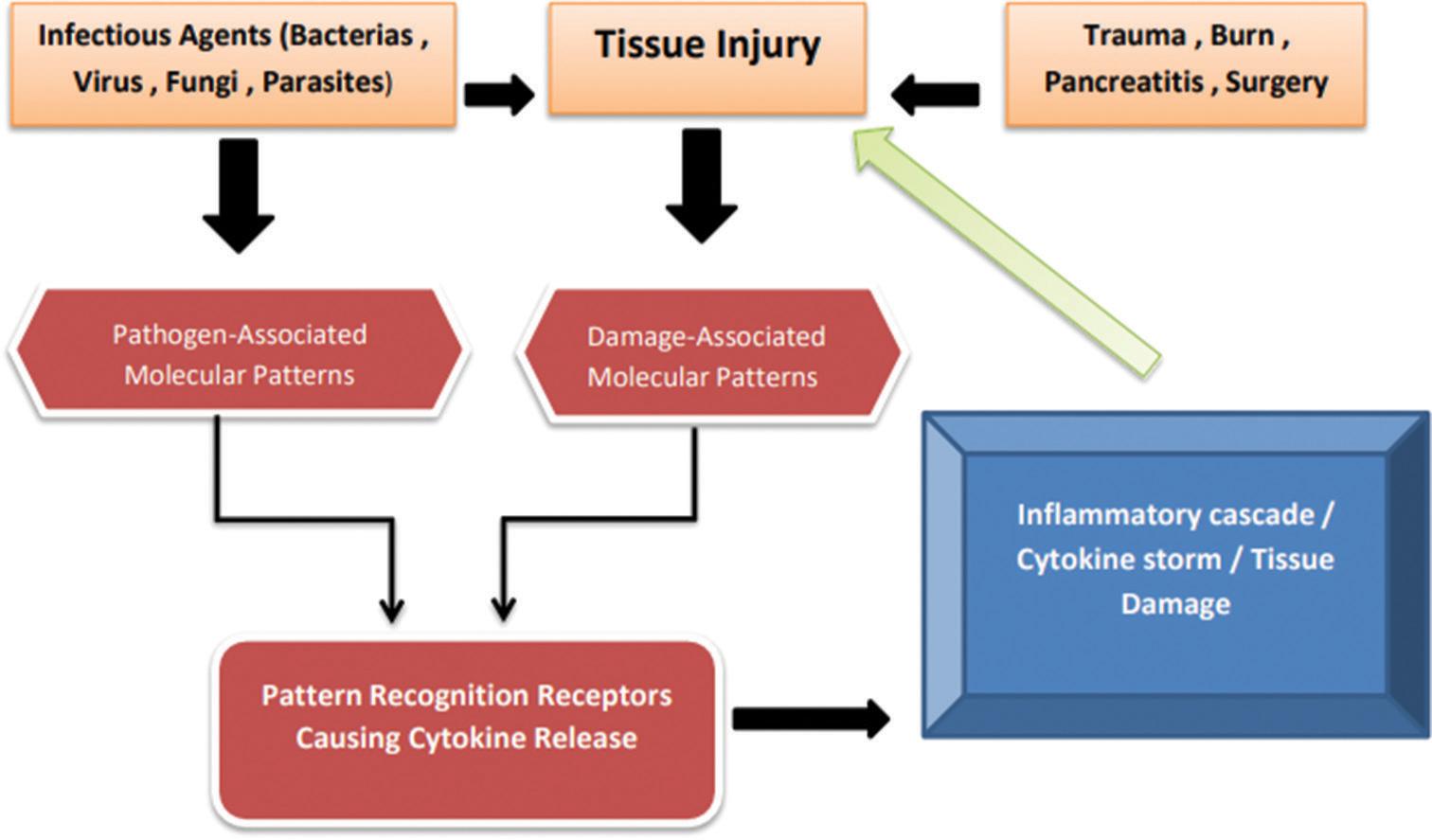
- Showing pathophysiology of sepsis and inflammatory cascade.
Management of cytokine storms includes elimination of exogenous and endogenous pathogenic triggers which cause abnormal activation of the immune system and maintain critical organ function through supportive care.[6] Furthermore, the use of extracorporeal adsorption of inflammatory mediators using specifically developed filters, adsorption membranes, haemoperfusion sorbent cartridges or columns has been suggested as one method to improve immune homeostasis in sepsis.
In the following article, we are going to review various extracorporeal therapies in sepsis.
Extracorporeal therapies are group of treatments which promote removal of endogenous or exogenous toxic substances and support or temporarily replace vital organs. It is used for various purposed such as dialysis, total plasma exchange, toxin removal and in sepsis.
In sepsis, it includes:
Removing endotoxin and PAMPs
Removing cytokines
Removing activated leukocytes
Removing pathogens
CUT OF MEMBRANES
It describes the smallest molecular weight of a solute that it retains. Low cutoff membranes are the membranes usually used for conventional haemodialysis which removes urea and creatinine. However, new membranes (i.e., medium cutoff and high cutoff membranes) with increased pore size have been developed for sepsis. These specialised membranes allow for the removal of higher molecular-weight molecules, such as inflammatory mediators, pathogenic organisms or the removal of nephrotoxic light chains of immunoglobulins. However, plasma proteins, such as albumin, are also filtered through this these membranes.[7]
PRINCIPLES
Adsorption
Convection
Table 1 shows various filters based on principle of adsorption and convection.
| Adsorption Based | Convection Based | Both |
|---|---|---|
|
|
|
FcMBL: Fc mannose binding lectin, CPFA: Coupled plasma filtration adsorption, HCO: High cutoff, LPS: Lipopolysacchride
ADSOPTION BASED
Toraymixin (Polymyxin B haemoperfusion cartridge)
Polymyxin B exerts its action by altering permeability and damaging bacterial cell membrane. It binds the lipid A portion of endotoxin, which is a toxic component of endotoxin and neutralises its toxicity. Polymyxin B as a cation binds with anionic lipid A portion. It is used cautiously in patients with renal failure due to its nephrotoxic effects. It is used with any of the dialysis machines with low blood flow 80–100 mL/min for the duration of 2 h, as filters get saturated. The main advantage of it is removal of endotoxin indirectly reducing further release of cytokines, but it has minimal cytokine clearance for the already formed cytokines and may lead to thrombocytopenia and granulocytopenia.[8] There are various trials done regarding these filters. Early use of polymyxin B hemoperfusion in abdominal sepsis (EUPHAS) trials, which were done in European Union and Italy, showed significant benefits in terms of mortality [Table 2].
| Trials and mortality Benefits | Sample size | Polymyxin B group (%) | Conventional group (%) |
|---|---|---|---|
| EUPHAS STUDY | |||
| Day 28 Mortality |
64 | 32 | 53 |
| EUPHAS 2 STUDY | |||
| Day 28 Survival |
357 | 75 | 39 |
| ABDOMIX STUDY | |||
| Day 90 Mortality |
232 | 33.6 | 24 |
| EUPHRATES STUDY | |||
| Day 28 Mortality |
449 | 37.7 | 34.5 |
EUPHAS: Early use of polymyxin B hemoperfusion in abdominal sepsis, EUPHRATES: Evaluating the Use of Polymyxin B Hemoperfusion in a Randomized Controlled trial of Adults Treated for Endotoxemia and Septic Shock
The EUPHAS trial suggested a positive outcome with improved haemodynamics, organ function scores and 28-day mortality in patients with intra-abdominal sepsis and septic shock treated with polymyxin B haemoperfusion.[9]
However, the ABDOMIX trial did not replicate these findings and even reported a slightly increased trend toward mortality in the intervention group. This discrepancy could be attributed to various factors such as differences in patient populations, trial design or variations in the administration of the intervention. The Evaluating the Use of Polymyxin B Hemoperfusion in a Randomized Controlled trial of Adults Treated for Endotoxemia and Septic Shock (EUPHRATES) multicentre trial, involving a larger number of patients with septic shock and elevated endotoxin levels, showed mixed results.
Alteco lipopolysacchride (LPS) adsorber device
It is also an endotoxin adsorber device which uses polyethylene discs with high affinity for lipid A (LPS) hydrophobic and ionic bonds. It is useful up to 2 h as its adsorber gets saturated. Various trials about this filter are as follows: none of them showed significant mortality benefits but improved softer end points [Table 3].
| Trial | Sample size | Significant findings |
|---|---|---|
| Yaroustovsky et al., trial 2009[10] | 13 | Improved MAP and endotoxin levels |
| AlaKokko et al., 2011[11] | 24 | Improved vasopressor requirement |
| Adamik et al., 2015[12] | 62 | Reduced endotoxin levels. |
MAP: Mean arterial pressure
CytoSorb
The CytoSorb haemoadsorption device is a medical tool designed to remove certain substances from the blood. It consists of small beads made of a material called polystyrene divinylbenzene copolymer. These beads have a large surface area of 45,000 square meters and can capture molecules up to a certain size (molecular cutoff size of 60 kDa). The primary function of CytoSorb is to adsorb or attract molecules involved in inflammation, both those that promote inflammation (pro-inflammatory) and those that regulate or dampen inflammation (anti-inflammatory). Notably, it does not remove endotoxins. In addition to inflammatory mediators, CytoSorb has demonstrated the ability to adsorb other substances such as myoglobin, bilirubin, bile acids as well as molecules such as PAMPs and DAMPs.[13]
A study conducted in 2013 in 2013 in 64 patients with septic shock reported a significant reduction in cytokine levels in the CytoSorb treatment group compared to the control group.
The intervention group also showed improvements in haemodynamics and organ function scores. Overall, there was a trend toward reduced 28-day mortality in the CytoSorb group, although the difference did not reach statistical significance.[14]
HA-330
Its resin-based cytokine adsorption filter gained popularity during COVID-19 pandemic. It has the special ability to adsorb C-reactive protein along with other inflammatory mediators. As it is saturated within 4 h, its usage is limited. According to a study conducted by M. A. Erkurt et al. in 2022 which was aimed to assess the effects of the HA-330 haemoperfusion cartridge, on haemodynamics, inflammatory cytokine levels, and mortality in critical care patients with severe sepsis, no significant effect was found.[15] In a randomised trial involving 44 patients, with 24 receiving HA-330 haemoperfusion and 20 receiving standard therapy, the study monitored parameters such as haemodynamics, haematology, coagulation function, organ function and sequential organ failure assessment scores on days 3, 7 and 14. The HA haemoperfusion group exhibited significant removal of IL-6 and IL-8, along with improved cardiac index, systemic vascular resistance index and reduced vasoactive agents compared to the control group at days 3 and 7. Although organ dysfunction showed no significant difference up to day 7, the haemoperfusion group demonstrated improvement by day 14. While 28-day mortality, hospital mortality and length of hospital stay showed no significant differences between the groups, intensive care unit (ICU) mortality and length of ICU stay were notably reduced in the HA group. The study suggests that HA haemoperfusion in sepsis is safe and may enhance organ function, decrease ICU mortality and shorten ICU stay, possibly attributed to the significant removal of inflammatory cytokines such as IL-6 and IL-8.
Fc mannose binding lectin (FcMBL)
The FcMBL haemoadsorption device is an extracorporeal therapy for sepsis that uses commercially available hollow fibre filters coated with a genetically engineered form of human opsonin FcMBL. This device efficiently removes a wide range of pathogens, including bacteria (Gram-negative and Gram-positive), fungi and endotoxins from circulating blood without the need to identify them beforehand. In in vitro tests with human blood, it demonstrated high removal rates (90–99%). In rat studies, FcMBL-hemofiltration (HF) significantly reduced circulating pathogens and endotoxins, preventing their accumulation in various organs. When used in conjunction with antibiotics, FcMBL-HF efficiently cleared microbial fragments, resulting in reduced organ pathogen and endotoxin loads, suppressed inflammation and improved vital signs compared to antibiotic treatment alone. This combined approach presents a promising strategy for more effective sepsis therapy.[16]
CONVECTION BASED DEVICES
High-volume HF (HVHF)
HVHF is an extracorporeal blood purification technique that involves removing a large volume of plasma water from the patient’s blood, along with solutes and inflammatory mediators. It is typically performed using a HF machine. During HVHF, a large volume of the patient’s blood is passed through a haemofilter and excess water and solutes are removed, creating a filtrate. The removed plasma water is replaced with a balanced solution to maintain fluid balance. It works on the principle of convection, that is transmembrane pressure gradient with solvent drag. It requires high flux dialyser.
In the IVOIRE trial, the results did not provide evidence supporting the use of HVHF at 70 mL/kg/h compared to contemporary standard-volume HF at 35 mL/kg/h in reducing 28-day mortality or facilitating early improvements in hemodynamic profile or organ function for patients with septic shock complicated by acute kidney injury (AKI). The application of HVHF, as studied in this trial, is not recommended for the treatment of septic shock with AKI based on the trial findings.[17]
In another review analysis, it incorporated three randomised trials encompassing a total of 64 participants. Among the trials, one provided data on ICU and 28-day mortality, another reported hospital mortality and discrepancies were noted in the reported mortality rates in the third trial. There were no mentions of ICU or hospital length of stay in any of the trials and only one trial provided information on organ dysfunction. Notably, adverse events were not documented across the studies.[18]
CONVECTION AND DIFFUSION
Coupled plasma filtration adsorption (CPFA)
CPFA represents an innovative extracorporeal blood purification therapy for sepsis, targeting the non-selective adsorption of both proinflammatory and anti-inflammatory mediators. In vitro investigations have confirmed the effectiveness of CPFA in adsorbing various inflammatory mediators, including IL-1β, IL-6, IL-8, IL-10 and tumour necrosis factor-α. Clinical studies have indicated that CPFA can enhance early haemodynamic stability, reduce the need for inotropic support and improve the immune response in septic patients. Despite these positive findings, the trials conducted thus far have not demonstrated any significant improvement in hard clinical outcomes.[19]
The COMPACT-2 trial assessed high-dose CPFA for septic shock treatment in 115 patients. The trial was halted due to potentially higher mortality in the CPFA group, particularly in the early septic shock phase. Patients not needing renal replacement therapy showed increased harm, with a dose-response effect observed. The study recommends against CPFA use in septic shock until underlying mechanisms are clarified.[20]
oXiris AN69
The oXiris membrane, an enhanced version of the AN69-ST membrane, serves a dual purpose by facilitating both cytokine adsorption and endotoxin removal during continuous renal replacement therapy (CRRT). Composed of sulfonate-containing polymers, its microporous structure aids in cytokine adsorption through cationic residues. The membrane is modified with polyethylenimine for enhanced endotoxin adsorption and pregrafted with heparin to improve antithrombotic properties. Overall, oXiris efficiently removes both cytokines and endotoxins in a single-membrane filter, making it a versatile option for CRRT.[21]
In a randomised crossover double-blind study, Broman et al.[22] found that, during the initial filter treatment, oXiris filter usage led to a significant decrease in endotoxin levels in 77.8% of patients, compared to 16.7% in the standard filter group. oXiris also demonstrated greater reductions in TNF-α, IL-6, IL-8 and interferon gamma, along with a decrease in lactate concentration, whereas the standard filter showed minimal changes. Norepinephrine infusion rates were reduced with oXiris CRRT but not with the standard filter. In the second treatment period, there were no significant reductions in endotoxin or cytokine levels in either group.[22]
The Seraph-100 microbind
The Seraph-100 microbind affinity blood filter is an extracorporeal haemoperfusion device designed to effectively bind and eliminate bacteria, fungi, viruses and cytokines from the blood. Using immobilised heparinised beads, it mimics the cell surface glycocalyx’s heparan sulphate, facilitating the binding and removal of pathogens and inflammatory cytokines, contributing to blood purification.[23]
In a study conducted by Stoffel et al.,[23] the Seraph-100 blood filter showed significant improvements in patients with septic shock and SARS-CoV-2 infection. After treatment, there were notable positive changes in mean arterial pressure, heart rate, oxygen levels, lactate levels and pH. Vasopressor requirements also decreased significantly for norepinephrine, vasopressin, dobutamine and angiotensin II. Overall, the use of the Seraph-100® filter demonstrated both statistical and clinical benefits in enhancing hemodynamic parameters and reducing vasopressor needs .[20]
CONCLUSION
Extracorporeal therapies present a significant advancement in the management of sepsis by focusing on the removal of harmful substances such as endotoxins, cytokines, activated leukocytes and pathogens. These therapies, including adsorption, convection and their combined approaches, show potential in restoring immune balance and supporting organ function in septic patients.
Adsorption-based therapies
Toraymyxin and Alteco LPS Adsorber are effective in removing endotoxins, thereby indirectly reducing cytokine levels.
CytoSorb and HA-330 target inflammatory mediators, with CytoSorb being capable of broader molecule adsorption and HA-330 proving beneficial during the COVID-19 pandemic.
FcMBL demonstrates a comprehensive approach by effectively eliminating a wide range of pathogens and endotoxins.
Convection-based therapies
HVHF, despite not showing significant mortality benefits, remains a critical component in the management of septic shock.
Combined adsorption and convection therapies
CPFA and oXiris AN69 provide dual functionalities, with CPFA focusing on inflammatory mediators and oXiris combining cytokine adsorption with endotoxin removal.
Seraph-100 Microbind Affinity Blood Filter has shown promise in improving hemodynamic parameters and reducing vasopressor needs, especially during SARSCoV-2 infection.
Although clinical trial results have varied, with some studies demonstrating significant benefits while others do not, the overall evidence suggests that extracorporeal therapies can improve hemodynamic stability, reduce inflammatory cytokine levels and support organ function. Further research is essential to optimise these therapies, elucidate their mechanisms and identify patient populations that will benefit the most. As technology and our understanding of sepsis evolve, extracorporeal therapies offer a hopeful prospect in improving outcomes and reducing mortality in this critical condition.
Ethical approval
The Institutional Review Board approval is not required.
Declaration of patient consent
Patient’s consent was not required as there are no patients in this study.
Conflicts of interest
There are no conflicts of interest.
Use of artificial intelligence (AI)-assisted technology for manuscript preparation
The authors confirm that there was no use of artificial intelligence (AI)-assisted technology for assisting in the writing or editing of the manuscript and no images were manipulated using AI.
Financial support and sponsorship
Nil.
References
- The Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3) JAMA. 2016;315:801-10.
- [CrossRef] [PubMed] [Google Scholar]
- Epidemiology of Sepsis and Septic Shock in Critical Care Units: Comparison between Sepsis-2 and Sepsis-3 Populations Using a National Critical Care Database. Br J Anaesth. 2017;119:626-36.
- [CrossRef] [PubMed] [Google Scholar]
- Cytokine Storm and Sepsis Disease Pathogenesis. Semin Immunopathol. 2017;39:517-28.
- [CrossRef] [PubMed] [Google Scholar]
- Cytokine Storm in COVID-19: The Current Evidence and Treatment Strategies. Front Immunol. 2020;11:1708.
- [CrossRef] [PubMed] [Google Scholar]
- Medium Cut-off Membranes-Closer to the Natural Kidney Removal Function. Int J Artif Organs. 2017;40:328-34.
- [CrossRef] [PubMed] [Google Scholar]
- Therapeutic Rationale for Endotoxin Removal with Polymyxin B Immobilized Fiber Column (PMX) for Septic Shock. Int J Mol Sci. 2021;22:2228.
- [CrossRef] [PubMed] [Google Scholar]
- Early Use of Polymyxin B Hemoperfusion in Abdominal Septic Shock: The EUPHAS Randomized Controlled Trial. JAMA. 2009;301:2445-52.
- [CrossRef] [PubMed] [Google Scholar]
- Preliminary Report Regarding the Use of Selective Sorbents in Complex Cardiac Surgery Patients with Extensive Sepsis and Prolonged Intensive Care Stay. Blood Purif. 2009;28:227-33.
- [CrossRef] [PubMed] [Google Scholar]
- A New Endotoxin Adsorber in Septic Shock: Observational Case Series. Blood Purif. 2011;32:303-9.
- [CrossRef] [PubMed] [Google Scholar]
- Endotoxin Elimination in Patients with Septic Shock: An Observation Study. Arch Immunol Ther Exp. 2015;63:475-83.
- [CrossRef] [PubMed] [Google Scholar]
- Extracorporeal Blood Purification Therapies for Sepsis. Blood Purif. 2019;47(Suppl 3):2-15.
- [CrossRef] [PubMed] [Google Scholar]
- A Multicenter Randomized Controlled Study of An Extracorporeal Cytokine Hemoadsorption Device in Septic Patients. Crit Care. 2013;17:62.
- [CrossRef] [Google Scholar]
- The Effect of HA330 Hemoperfusion Adsorbent Method on Inflammatory Markers and End-Organ Damage Levels in Sepsis: A Retrospective Single Center Study. Eur Rev Med Pharmacol Sci. 2022;26:8112-7.
- [Google Scholar]
- Improved Treatment of Systemic Blood Infections Using Antibiotics with Extracorporeal Opsonin Hemoadsorption. Biomaterials. 2015;67:382-92.
- [CrossRef] [PubMed] [Google Scholar]
- High-volume Versus Standard-volume Haemofiltration for Septic Shock Patients with Acute Kidney Injury (IVOIRE Study): A Multicentre Randomized Controlled Trial. Intensive Care Med. 2013;39:1535-46.
- [CrossRef] [PubMed] [Google Scholar]
- High-volume Haemofiltration for Sepsis. Cochrane Database Syst Rev. 2013;1:CD008075. Update in: Cochrane Database Syst Rev 2017;1:CD008075
- [CrossRef] [Google Scholar]
- Coupled Plasma Filtration and Adsorption (CPFA): A Single Center Experience. Nephrourol Mon. 2013;5:891-6.
- [CrossRef] [PubMed] [Google Scholar]
- High Dose Coupled Plasma Filtration and Adsorption in Septic Shock Patients. Results of the COMPACT-2: A Multicentre, Adaptive, Randomised Clinical Trial. Intensive Care Med. 2021;47:1303-11.
- [CrossRef] [PubMed] [Google Scholar]
- Extracorporeal Therapy in Sepsis. Indian J Crit Care Med. 2020;24(Suppl 3):S117-21.
- [CrossRef] [PubMed] [Google Scholar]
- Endotoxin and cytokine reducing properties of the oXiris membrane in patients with septic shock: A randomized crossover double-blind study. PLOS ONE. 2019;14:e0220444.
- [CrossRef] [PubMed] [Google Scholar]
- Single-Center Experience with the Seraph-100® Microbind® Affinity Blood Filter in Patients With SARS-CoV-2 Infection and Septic Shock at a Military Treatment Facility. Mil Med. 2023;188:e2670-4.
- [CrossRef] [PubMed] [Google Scholar]




